Wound Location Chart
Wound Location Chart - Type of wound (if known) degree of tissue damage. Wounds should be assessed and documented at every dressing change. Damage or disruption of living tissue's cellular, anatomical, and/or functional continuum defines a wound. List six factors to consider when assessing darkly pigmented skin. Wound location, etiology, classification or stage, size of wound (length, width, and depth), amount of wound tunneling and undermining, types of tissues and structures observed in the. Presence of foreign bodies ; Review (if indicated) all support surfaces and positioning devices used to manage the patient’s tissue load. Web for the patient who has a wound: Provide accurate communication and documentation. Wound location should be documented using the correct anatomical terms—for example, right greater trochanter rather than right hip. Provide accurate communication and documentation. Wound location should be documented using the correct anatomical terms—for example, right greater trochanter rather than right hip. Presence of foreign bodies ; Download the access app here: Place a check in the box that represents the wound type: Nurses must also document the location and depth of any tunneling or undermining. We have a new app! Web wound location, described with proper anatomical terms. Provide accurate communication and documentation. Review (if indicated) all support surfaces and positioning devices used to manage the patient’s tissue load. Nonblanchable erythema of intact skin 5 stage 2. It’s important to document tissue type (slough, eschar, epithelial, granulation, etc.),. Web this highlights the importance of wound classification systems specific to each medical specialty. Wound edges and periwound skin. Web all patients with a nonhealing lower extremity ulcer should have a vascular assessment, including documentation of wound location, size, depth, drainage,. This document contains information on the following: Web many components of the assessment should be included in weekly documentation through a nurse's narrative note or a wound assessment chart: Wound edges and periwound skin. Abdomen, knee, coccyx, sacrum, trochanter (hip), ischial tuberosity (buttock), calcaneus (heel), malleolus (ankle), etc. Indicate whether or not the patient developed the wound while in hospital. Web wound location, described with proper anatomical terms. List six factors to consider when assessing darkly pigmented skin. Surface area = length x width. Include length, width, and depth. A layer that contacts the wound, and a layer that is adhesive that. What kind of wound is it? We have a new app! • tips for recording location • reference guide to anatomical terminology. Review all clinician consultations related to specialty management programs for skin and wound care. Wound dehydration or maceration) stable temperature (approximately 37 o c) neutral or acidic ph; Presence of foreign bodies ; The swc system was established when all surgical procedures were conducted openly. Download the access app here: List six factors to consider when assessing darkly pigmented skin. Granulation, slough, or necrotic tissue? Note amount of exudate, color, consistency, and odor. Download the access app here: Type of wound (if known) degree of tissue damage. Web identify wound location to: Presence of foreign bodies ; Web all patients with a nonhealing lower extremity ulcer should have a vascular assessment, including documentation of wound location, size, depth, drainage, and tissue type; List six factors to consider when assessing darkly pigmented skin. Maceration (softening of tissues by soaking in fluids) Wounds should be assessed and documented at every dressing change. Web this highlights the importance of wound. What kind of wound is it? • tips for recording location • reference guide to anatomical terminology. Nurses must also document the location and depth of any tunneling or undermining. Web all patients with a nonhealing lower extremity ulcer should have a vascular assessment, including documentation of wound location, size, depth, drainage, and tissue type; Web identifying wounds by anatomical. Include length, width, and depth. This method uses wound tracing sheets comprised of two layers: This document contains information on the following: Due to damage of underlying soft tissue from pressure and/or shear. Web identifying exactly where on the body a wound is located, as well as the type of wound, will determine treatments used and interventions instituted. Wound dehydration or maceration) stable temperature (approximately 37 o c) neutral or acidic ph; Nonblanchable erythema of intact skin 5 stage 2. Web wound location, described with proper anatomical terms. These systems can effectively categorize wounds based on injury severity, location, and patient comorbidities. Abdomen, knee, coccyx, sacrum, trochanter (hip), ischial tuberosity (buttock), calcaneus (heel), malleolus (ankle), etc. In the second part of our documenting wounds series, we look at how to document where a wound is located in relation to the body part. The location of the wound should be recorded accurately. Presence of foreign bodies ; Wound location, etiology, classification or stage, size of wound (length, width, and depth), amount of wound tunneling and undermining, types of tissues and structures observed in the. Web identify wound location to: Designate left, right, top, bottom, side, front, middle, etc., as appropriate (for example, inner left knee) describe anatomical location according to your facility practice;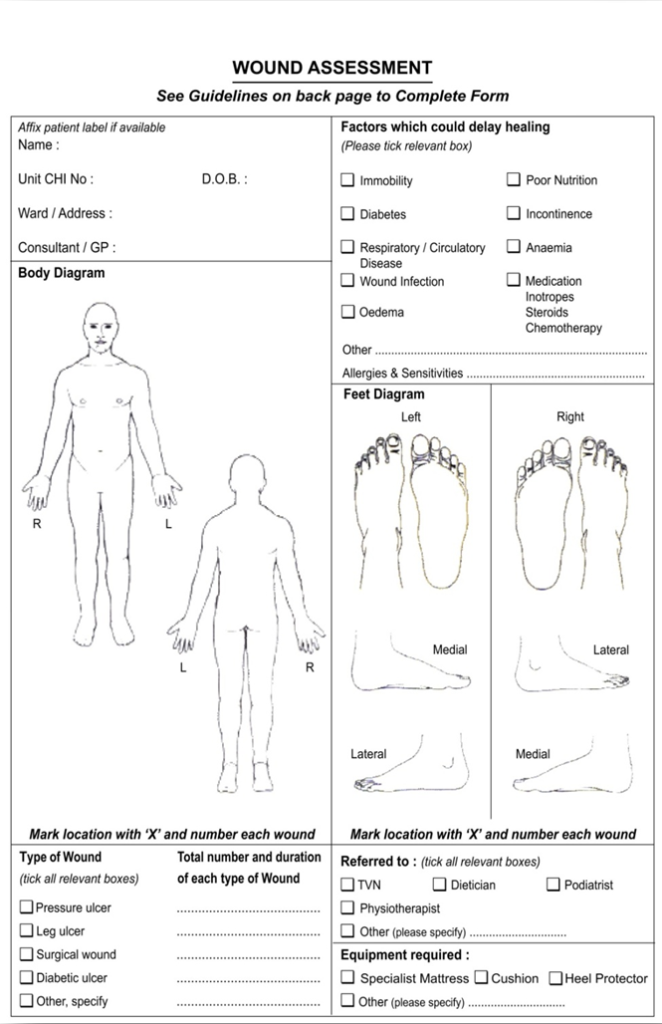
Wound Location Chart

Wound Location Chart

Pressure Ulcer Location Diagram Body Injury Diagram Body map

Health Care Patient comfort, Wound care, Acute care

common pressure sore locations的圖片搜尋結果 Wound care, Pressure ulcer
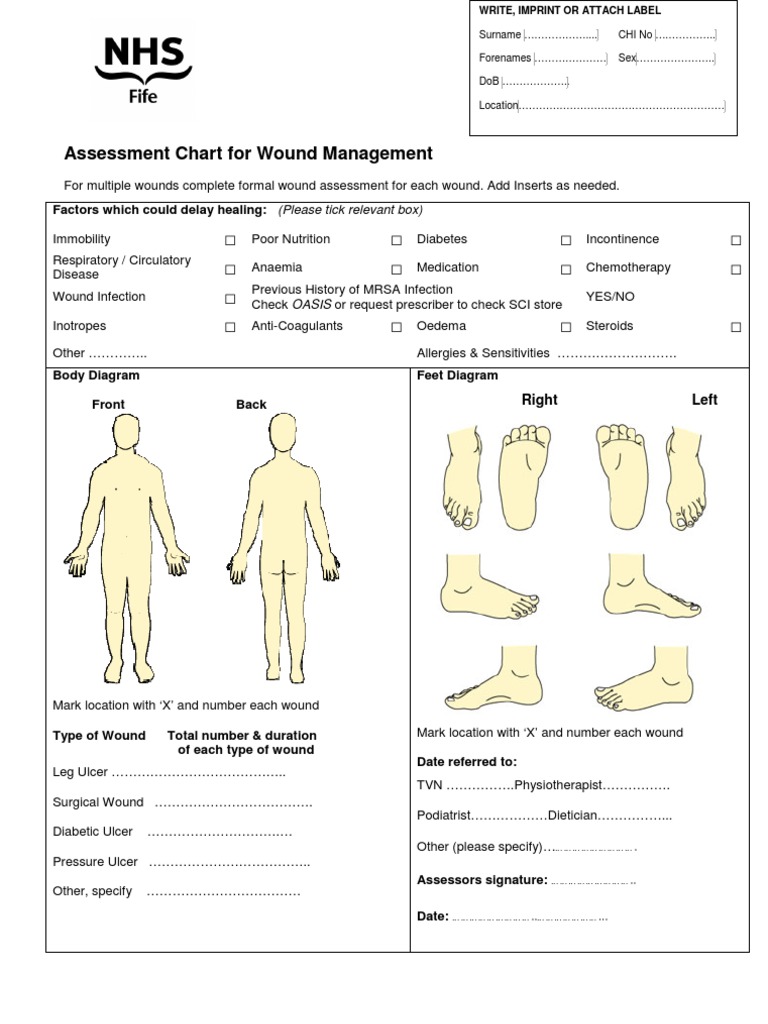
NHS Fife Assessment Chart for Wound Management Wound Clinical Medicine

Anatomical Charts and Posters Anatomy Charts Geriatric Health
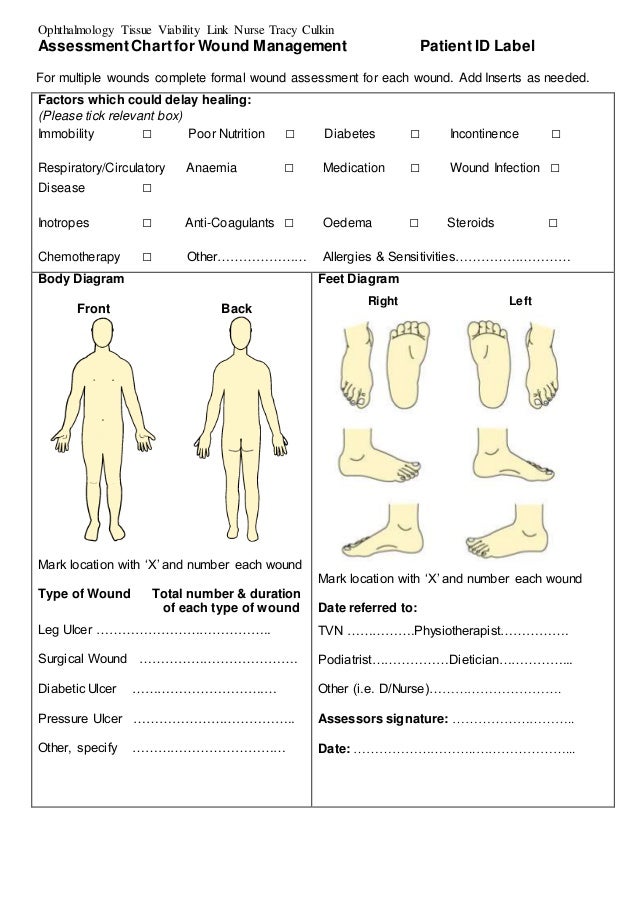
Assessment Chart for Wound Management Patient ID Lab…
Wound Assessment Chart.pdf Wound Allergy

Diagram showing typical sites of accidental injury, contrasted with
Web Wound Management Practices And Moisture Balance (E.g.
Web Location And Age Of Wound.
Include An Anatomical Figure Or Diagram Of The Human Body, With The Wound’s Location Noted In Your Assessment Record To Provide Complete Admission Documentation.
Wound Edges And Periwound Skin.
Related Post: